The area of parotid deep to the facial nerve is considered the deep lobe. Roughly 20% of parotid tumors happen to be deep to the facial nerve and as such 20% of tumors are deep lobe tumors.
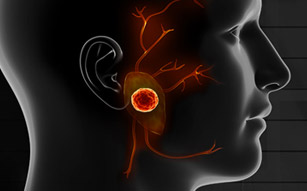
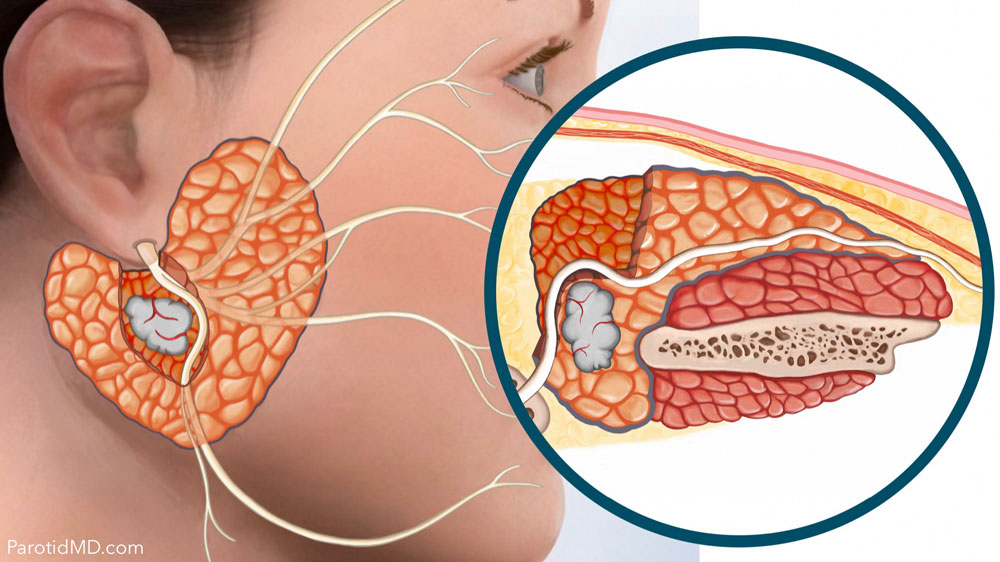
Cross section of the parotid Gland
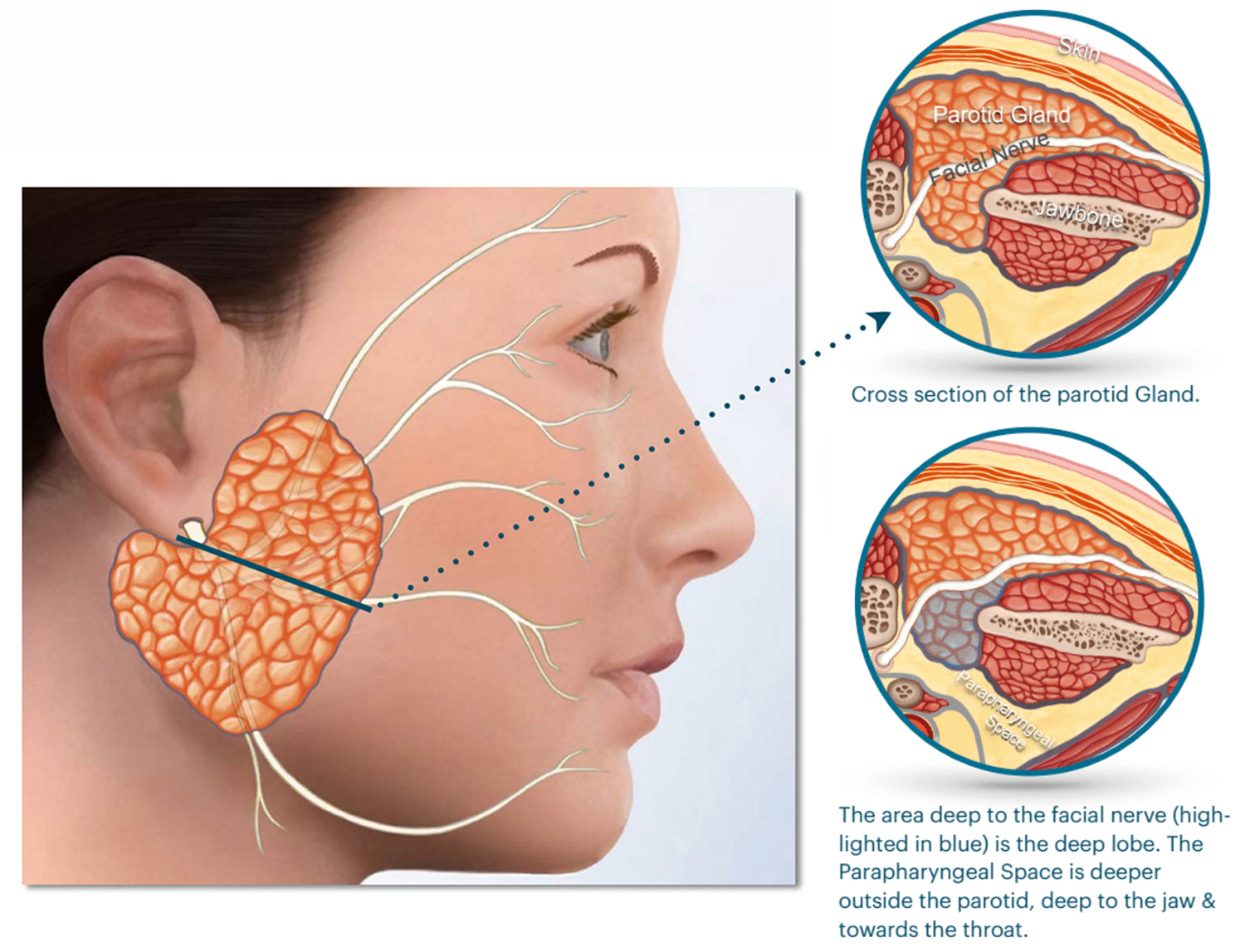
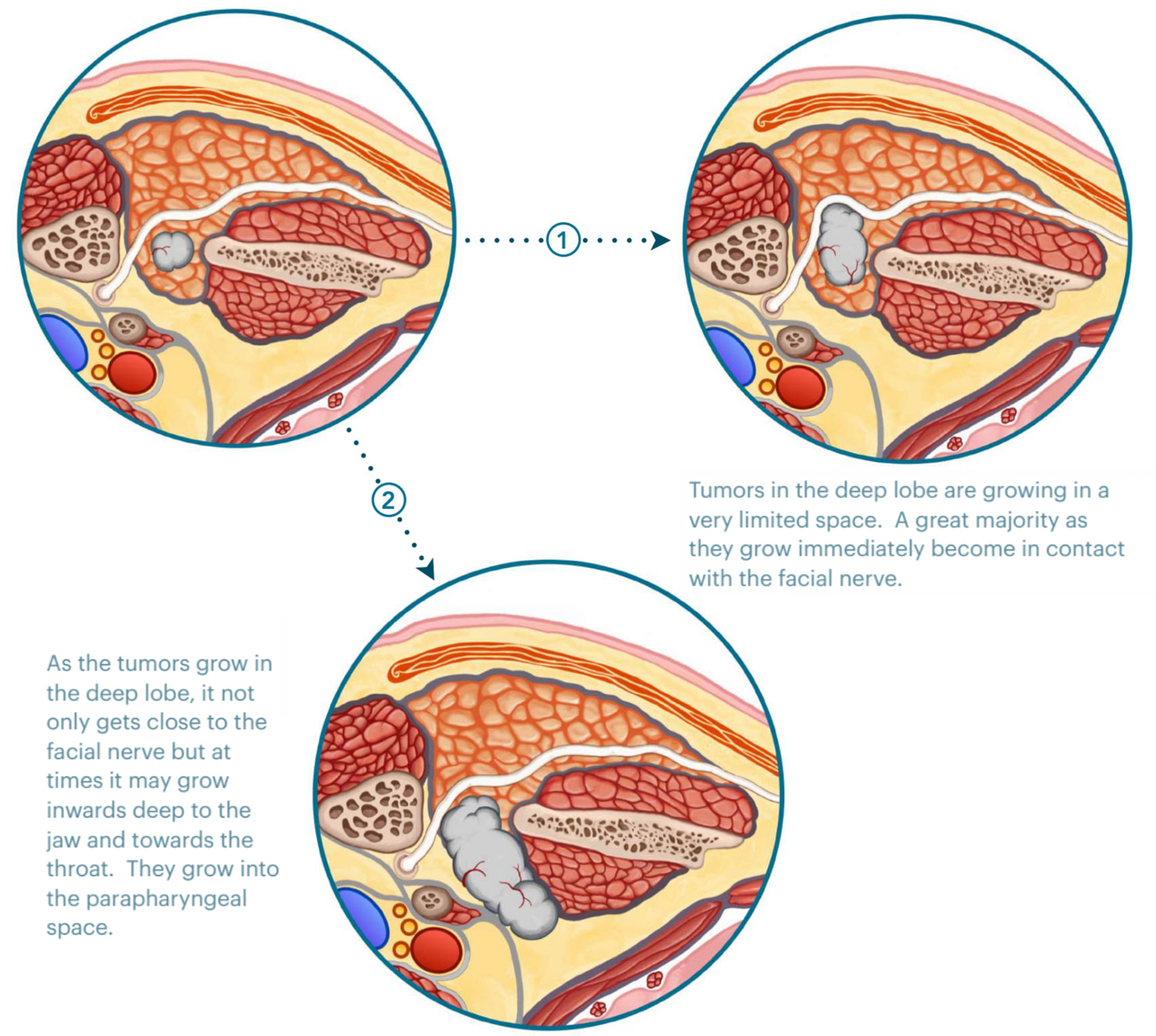
Tumors in the deep lobe fall into 2 categories:
- Tumors that start in the deep lobe and stay in the parotid gland.
- Tumors that start in the deep lobe and extend deeper into the parapharyngeal space.
MICRO-PAROTIDECTOMY FOR A DEEP LOBE TUMOR
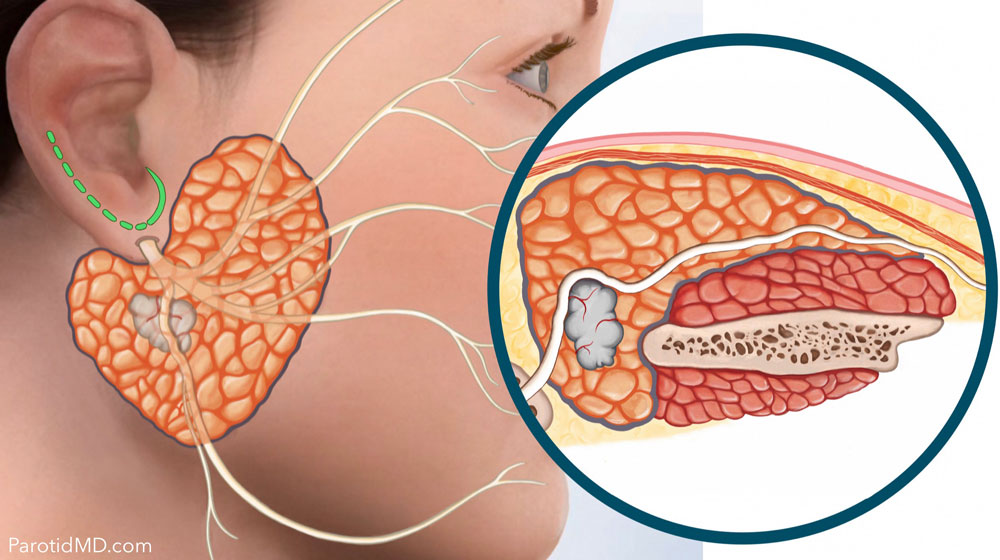
The tumor is deep to the facial nerve, and as it has grown, it has started to push & move the nerve. The nerve continues to work perfectly as long as the tumor only pushes on the nerve slowly (most benign tumors) and does not invade the nerve(possibly with cancers). The Micro-parotidectomy incision (marked in green).
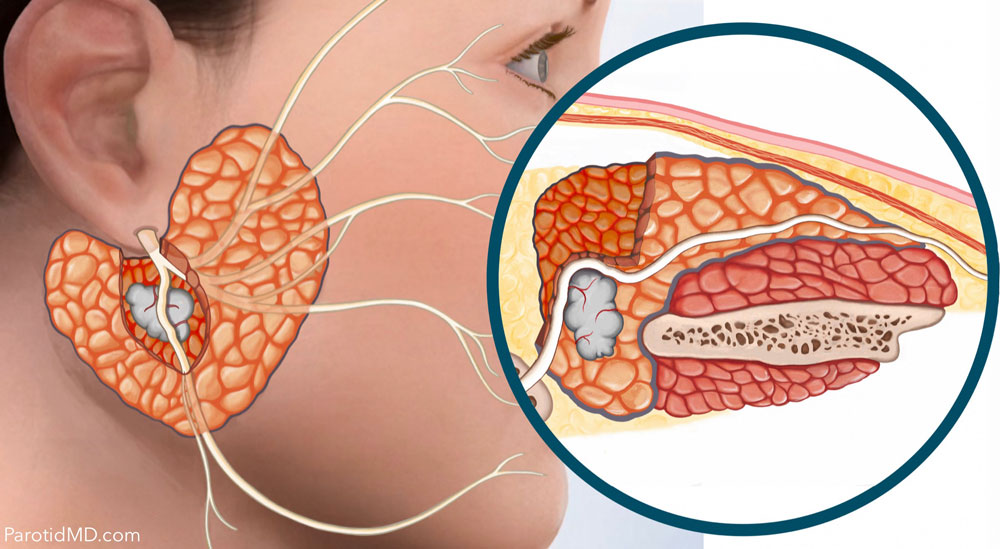
The main facial nerve, and some of the branches in the vicinity of the tumor, are identified, then clearly & gently exposed.
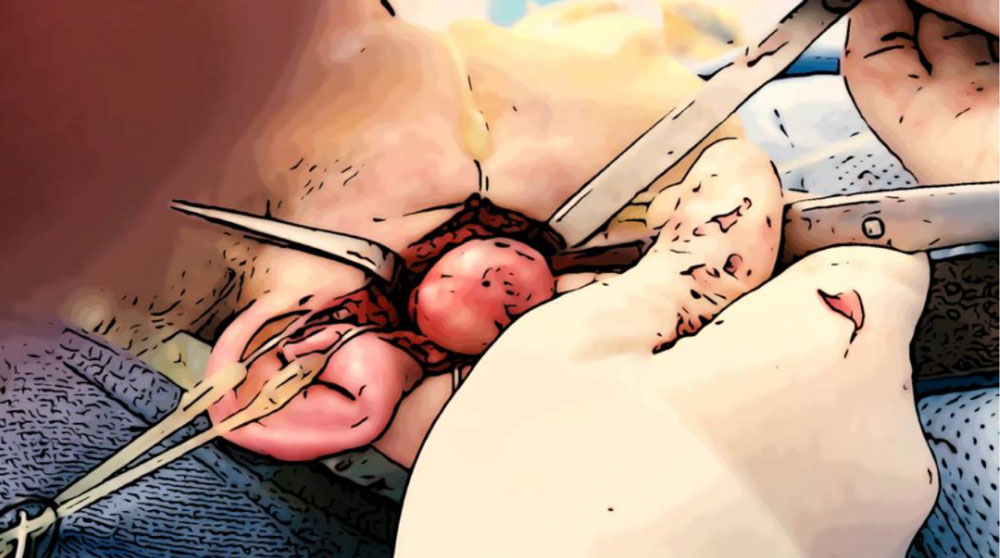
The tumor is now further examined, felt & its attachment to the surrounding tissue assessed.
The plane between the facial nerve & the tumor is identified; the nerve is gently separated and moved out of the way. If there is more space separating the tumor & nerve, then the tumor is removed from under the nerve without manipulating the nerve.
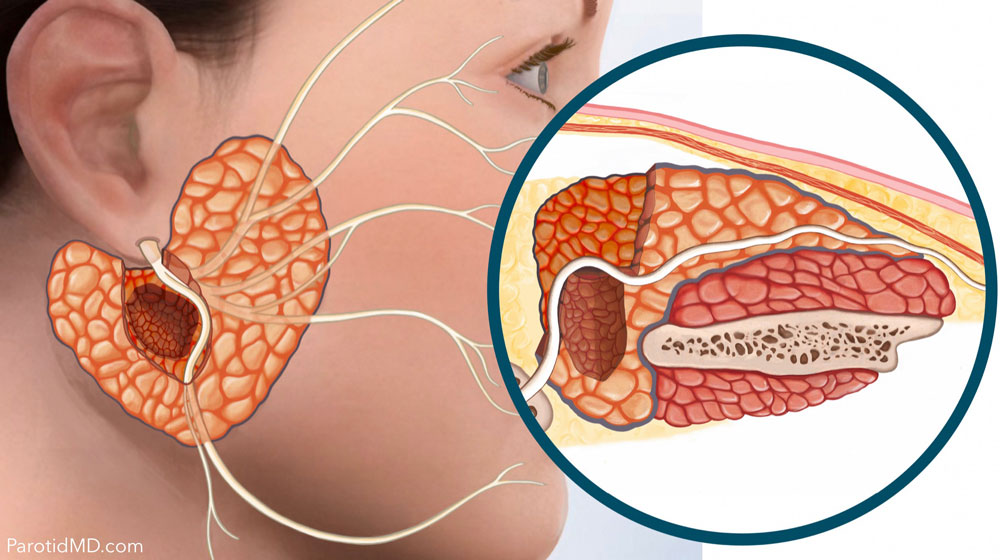
The tumor and an appropriate amount of healthy parotid tissue surrounding it are removed from the deep lobe. This is to prevent a recurrence of the tumor in the future.
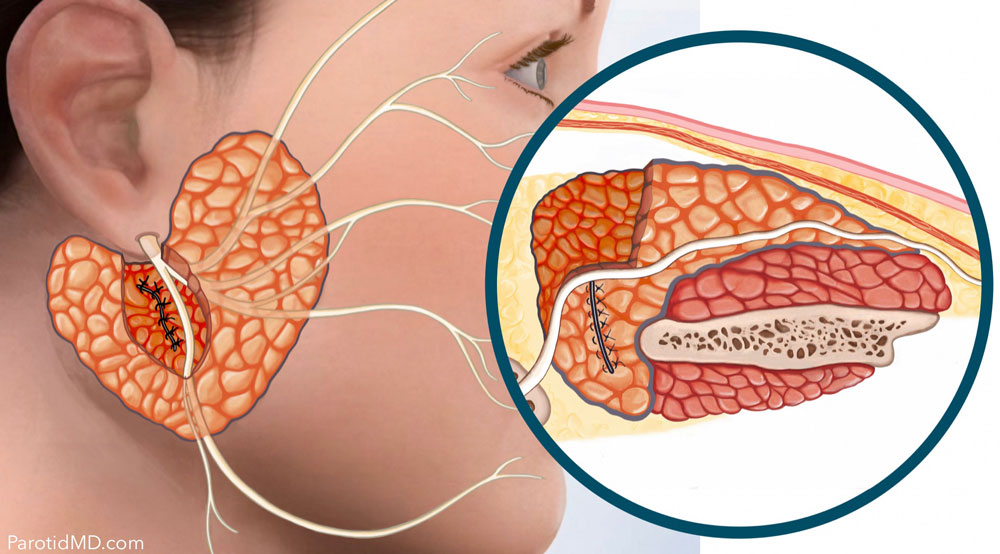
The remaining parotid tissue in the deep lobe is brought together and sutured. The facial nerve will then be placed in the position that has no tension on the nerve.
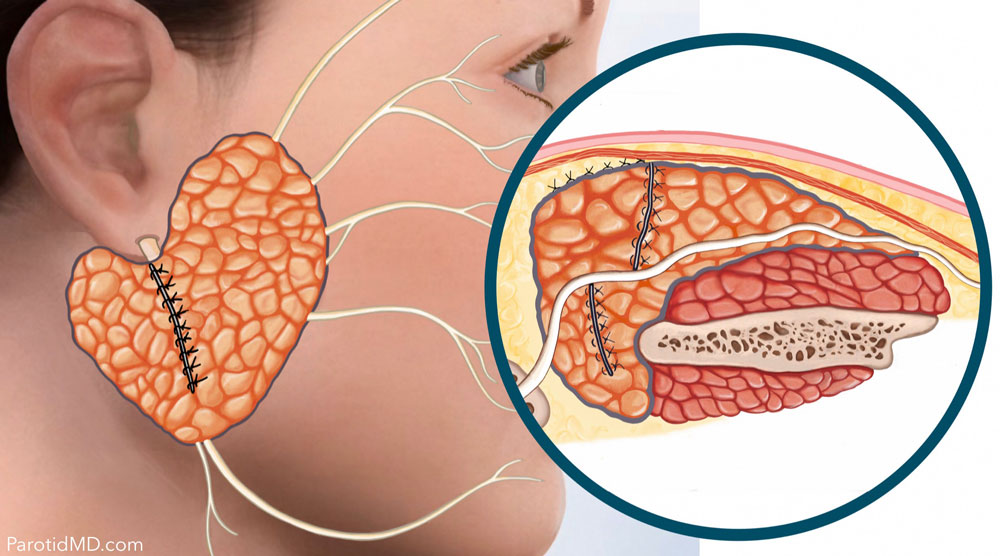
The superficial parotid of the parotid is also brought together & sutured. Then the SMAS layer and skin are laid back down onto the surface of the parotid. This will create facial symmetry & smooth contouring.

The whole procedure is done through the micro-parotidectomy approach. The incisions are closed with fine plastic surgery sutures to allow them to heal well and fade.
All of this is not only to reconstruct the parotid and create symmetry in the face, but also to prevent Frey’s Syndrome.
This is an outpatient procedure & does not require hospitalization.
FREQUENTLY ASKED QUESTIONS
Does deep lobe micro-parotidectomy need to be performed at a hospital, and does it require overnight stay at the hospital?
The answer to both questions is no. This is an outpatient procedure for the majority of patients. The only exceptions are patients who have other medical problems such as heart, lung or kidney disease that requires more medical attention and monitoring for these particular organs rather than the parotid surgery itself.
Are the facial nerves monitored during deep lobe parotidectomy?
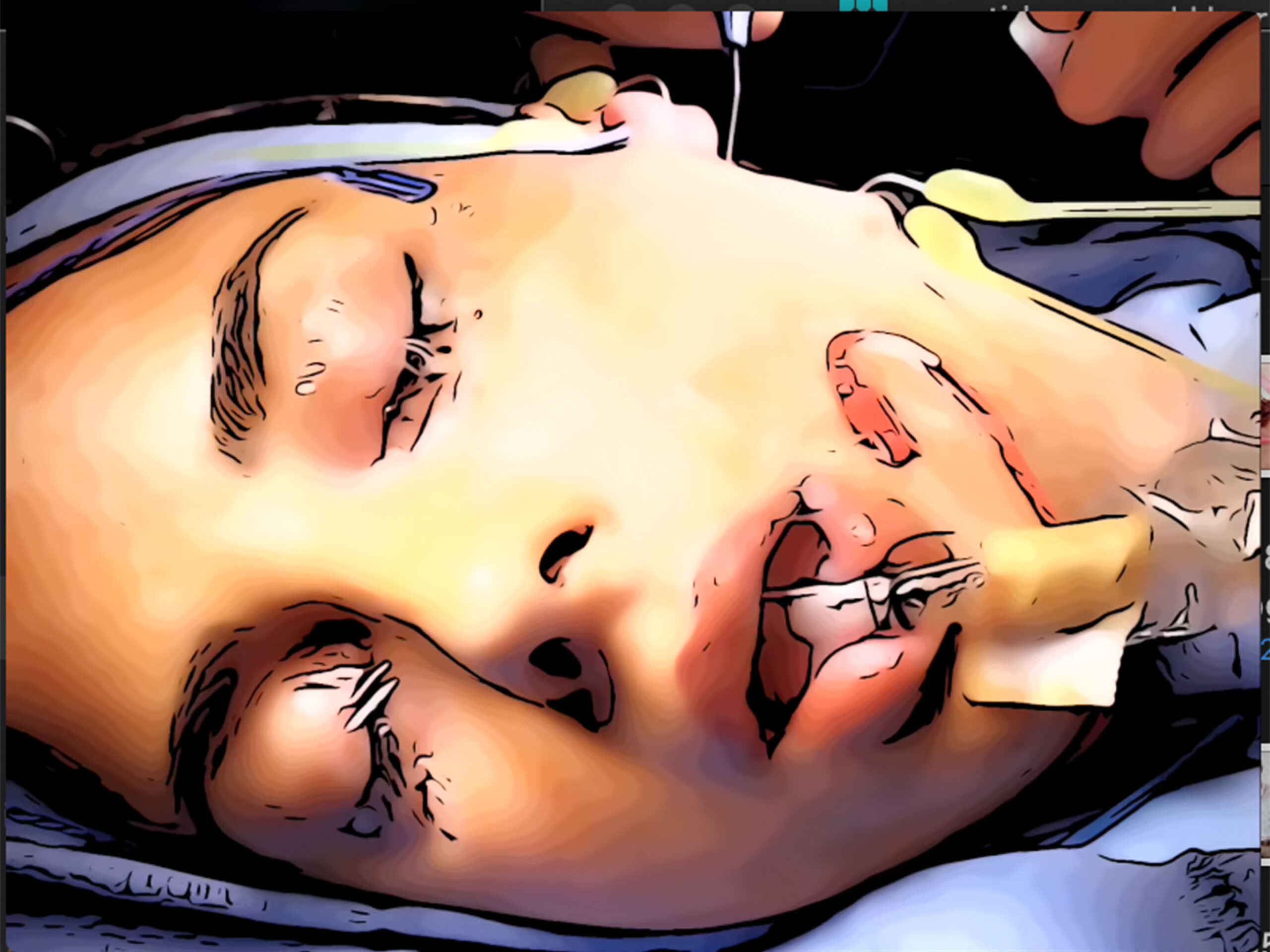
Yes, in every single case a facial nerve monitoring system is used. This system continuously checks the activity of the facial nerve. When it senses the slightest activity close to the nerve it sends alerts. It alerts the surgeon that they are close to the nerve and to exercise extreme caution. This is no substitute for expertise but is an additional measure of safety for the nerve. In the video the monitors can be seen as blue probe, next to the eye & red probe for the lip.
What other measures are taken to assure the integrity of the facial nerve during deep lobe micro-parotidectomy?
After all the facial nerve branches in the area of the surgery are identified and then the tumor removed; then each of the branches of the facial nerve are stimulate with a Checkpoint nerve stimulator to make sure each branch is working to definitively confirm during surgery that the facial nerves are intact and functioning.
STIMULATION OF THE FACIAL NERVES AFTER REMOVING THE TUMOR TO ASSURE ALL BRANCHES ARE WORKING (converted into animation)
Are any of the branches of the facial nerve cut during micro-parotidectomy?
Absolutely not. The facial nerve is too important for any of its branches to be compromised. Majority of the time during this surgery is spent on identification of the facial nerve and its branches Facial nerve expertise is of vital importance as is attention to detail and patience. There is no reason to not take extra time to try to preserve every single branch of this vital nerve. In addition, for deep lobe tumors, it is essential that your surgeon is extremely skilled & gentle; by nature of their location the tumor is deeper then the facial nerve and the nerves must be gently separated from the tumor and then the tumor removed. The more experienced & gentle the surgeon, the more likely it is to preserve the nerve without the slightest swelling or bruising, thus allowing the nerve to function better.
Are the tumor in the deep lobe of the parotid more likely to be cancerous?
Fortunately not. Close to 80% are benign just like the rest of the parotid gland areas. Only 20% are cancers.
Are deep lobe tumors more likely to recur or come back?
That has all to do with the expertise of your surgeon. The tumors are the same in terms of aggressiveness of behavior in the superficial and the deep lobes, but the deep lobe has a lot less space and more proximity to the facial nerve There is less additional healthy parotid tissue that can be taken to minimize recurrence. But in the hands of an expert surgeon the risks are very much minimized.
What percentage of patients get Frey’s syndrome after micro-parotidectomy?
Significantly less than 1%, mainly because all patients have parotid reconstruction & the SMAS layer is preserved that separates the parotid from the skin. This separation is the key to prevention of Frey’s syndrome.
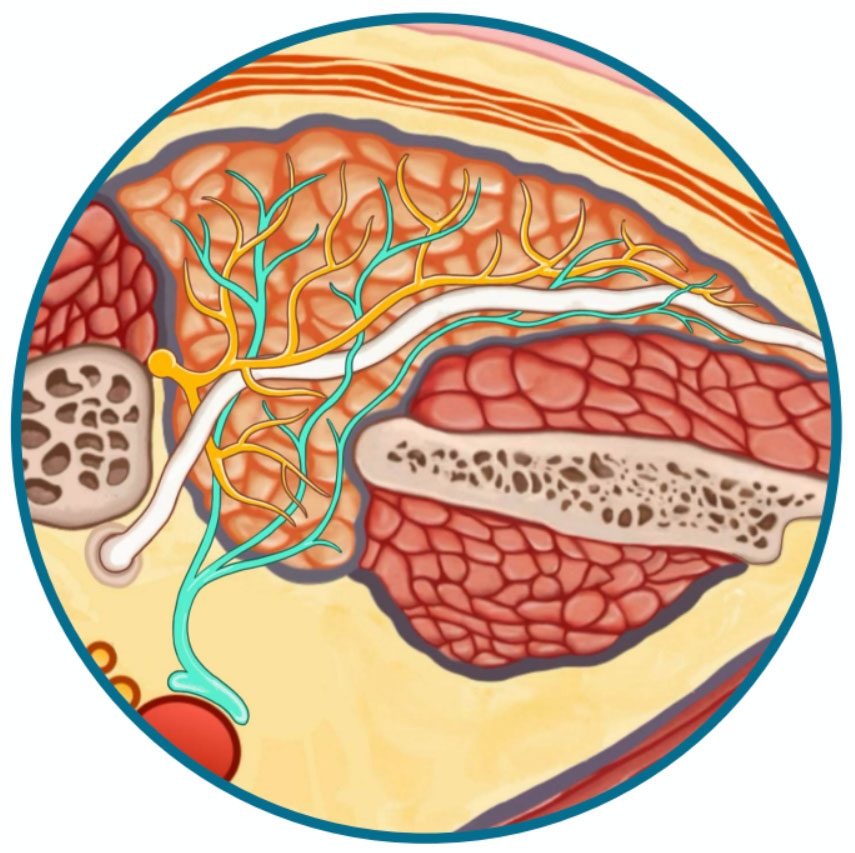
What is First Bite Syndrome?
Besides the facial nerve there are 2 other much smaller nerves that come into the parotid & control production and release of saliva. One set of microscopic nerve branches come from Auricotemporal Nerve that tell the gland to produce & squeeze out saliva (dark yellow); the other are set of very small nerves that come from the area deep to the parotid gland (light green – Sympathetic Nerve branches that travel with the carotid artery) and come in the gland and counter act the effects of the Auricotemporal Nerve. So the two nerves balance each other. If a tumor in the deep lobe either involves the Sympathetic Nerve branches or if during surgery a lot of these nerve branches are removed along with the tumor, then the Auricotemporal Nerve works without the counterbalance of the Sympathetic Nerves and therefore cause the parotid gland to squeeze hard during the first bite of the meal. The pain is instantaneous and stops with the rest of the bites of the meal. In most cases, this problem resolves over time.
Can deep lobe micro-parotidectomy be done for out of town patients?
Yes. In fact more then 90% of parotid surgeries done at the CENTER are for patients traveling from out of town or other countries. The complication rates during and after surgery are exceedingly low and so there is only a 5 day post surgery observation period when you may need to remain in town and be seen by Dr. Larian (usually 2-3 visits after surgery during the 5 days). The plastic surgery sutures are very fine, absorbable and under the surface; thus there is no suture to be removed. In short, the surgery and recovery from micro-parotidectomy is planned for patients to only have a very short stay in Los Angeles.
Is there more then one surgeon present during deep lobe micro-parotidectomy?
Majority of parotidectomies and reconstructions are performed by Dr. Larian alone. The more complex cases with larger or more aggressive tumors may require the assistance of Dr. Azizzadeh, especially if there is a concern for the health of the facial nerve, or if there is very complicated reconstruction to be done. Dr. Slattery is an Otologist (ear surgery specialist) who helps with surgery when the tumor is sitting against the skull and wont allow easy identification of the facial nerve. In this case Dr. Slattery will find the facial nerve in the bone behind the ear and allows us to more safely separate the nerve from the tumor.
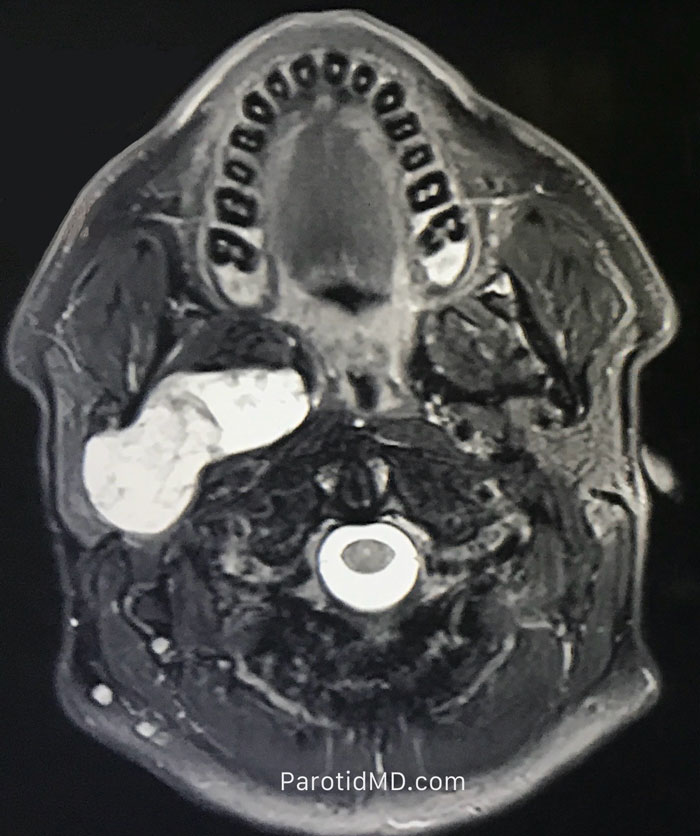
Can large deep lobe tumors that extend into the parapharyngeal space be removed through the micro-parotidectomy approach?
Yes. In fact, it’s the preferred method at the CENTER. In the MRI images to the right you see a large tumor (bright white) starting from the parotid and pushing into the throat. However, on MRI the tumor appears to be in the area where the facial nerve enters and courses through the parotid. As such, it is imperative that the tumor be removed after the facial nerve and the branches are identified to assure they remain safe In the animated video of the live surgery below you can see the large tumor seen on MRI being brought out through the micro-parotidectomy approach. This is followed by reconstruction of the area.

Meet The Team
Led by board-certified parotid surgeon, Dr. Babak Larian, our team of specialists has decades of experience successfully diagnosing and treating diseases of the parotid glands with minimally invasive procedures. Distinguished by our compassionate care and cutting-edge techniques, the CENTER has developed a reputation for delivering the best parotid tumor surgery available.