TYPES OF CANCEROUS TUMORS
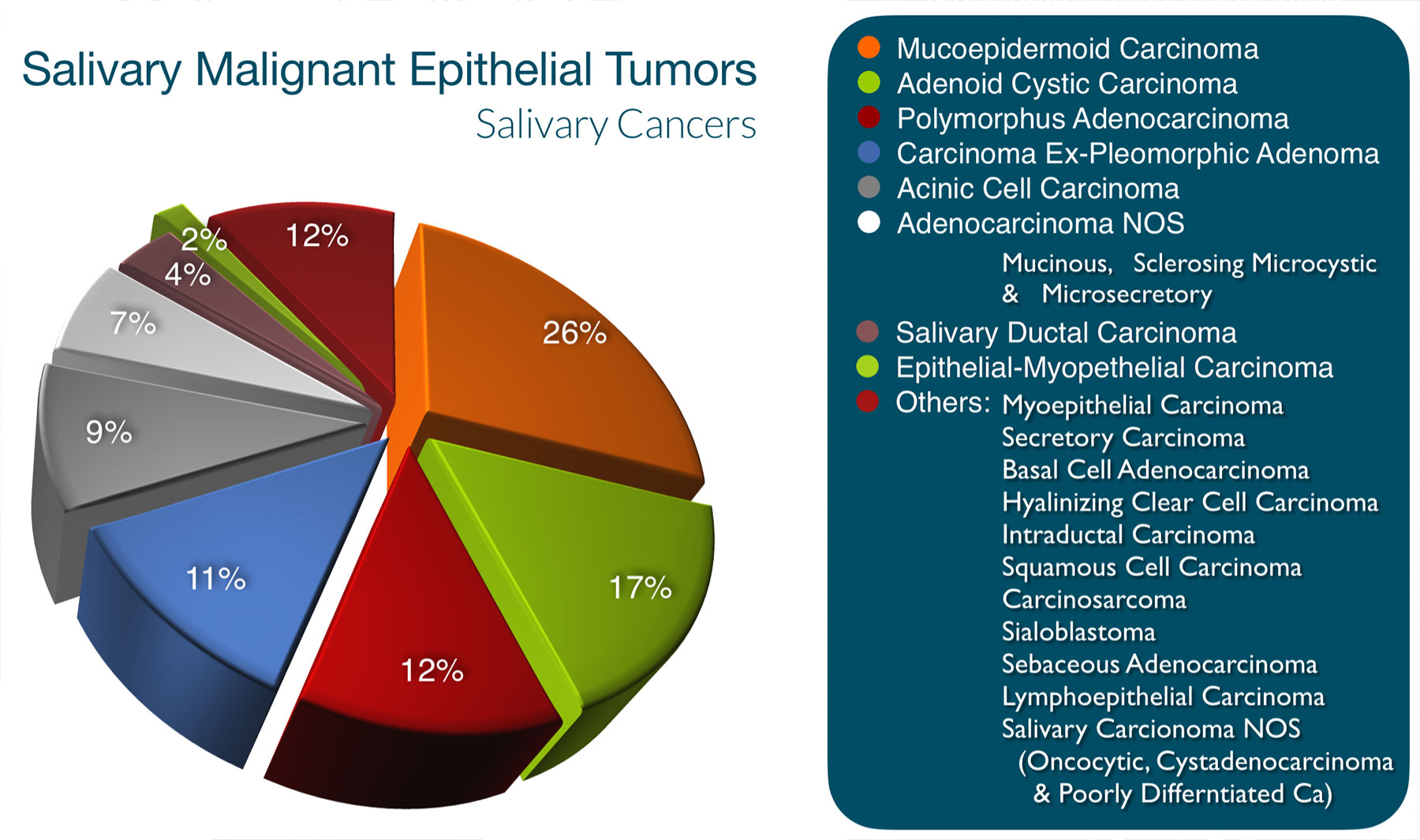
There are 21 different types of malignant tumors (aka cancers) that occur in the salivary glands. The difference between benign & malignant (cancerous) tumors is that benign tumors don’t tend to spread & generally don’t eat through adjacent structures, but rather, as they grow, push on the tissue next to them. Cancers can both invade and destroy adjacent structures (nerve, muscle, bone, blood vessels, etc) and can spread to lymph nodes and other parts of the body (lung, liver, bones, etc.).
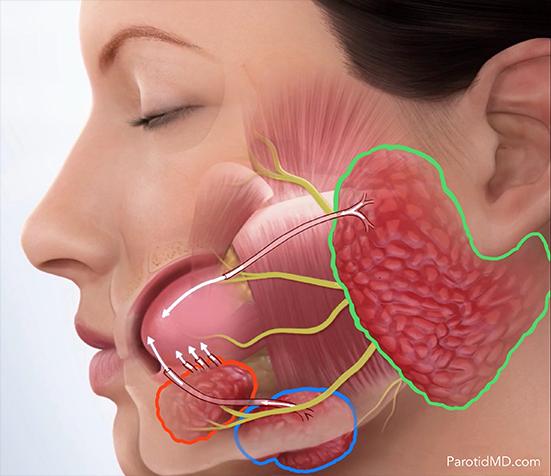
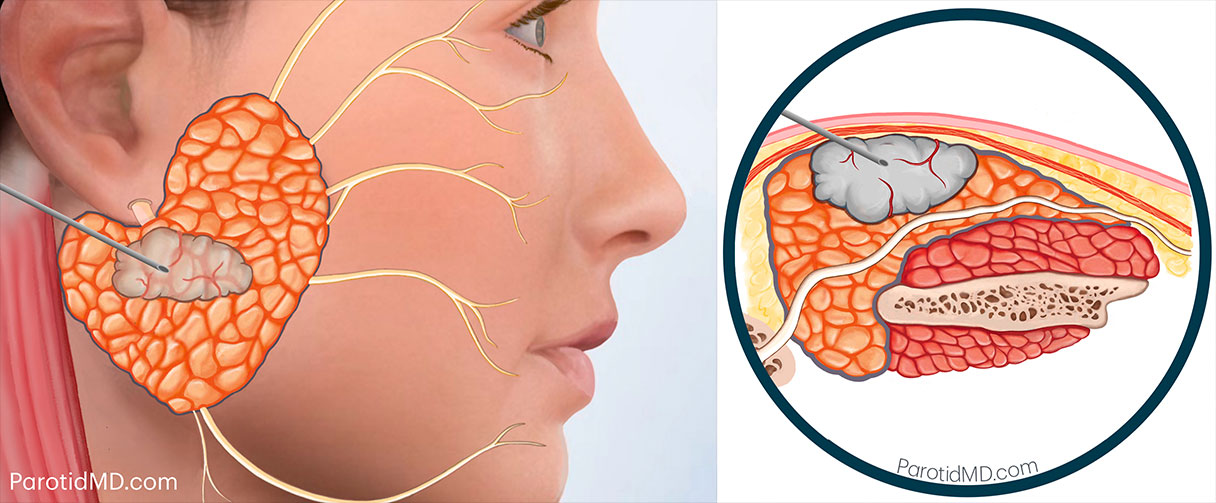
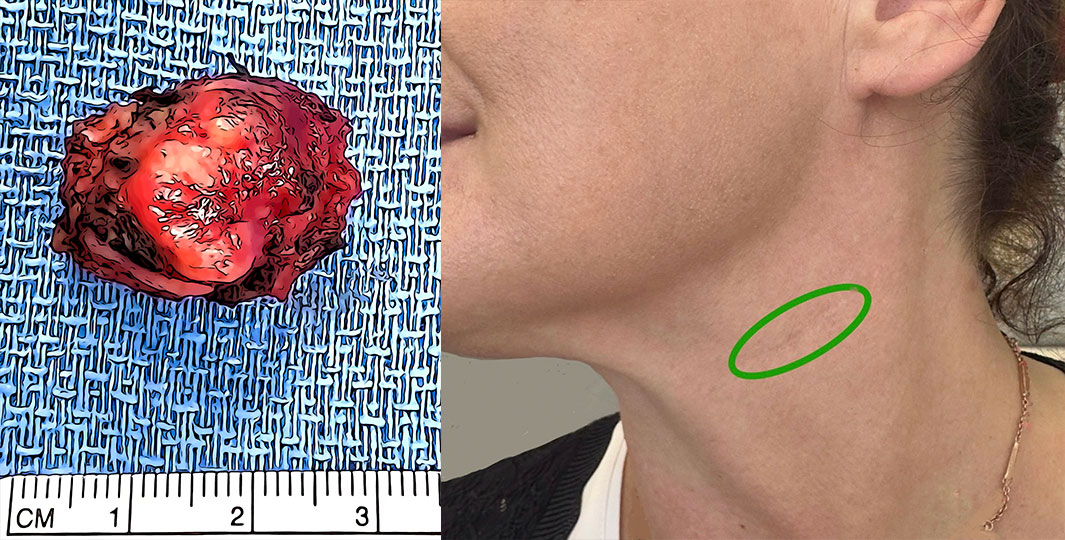
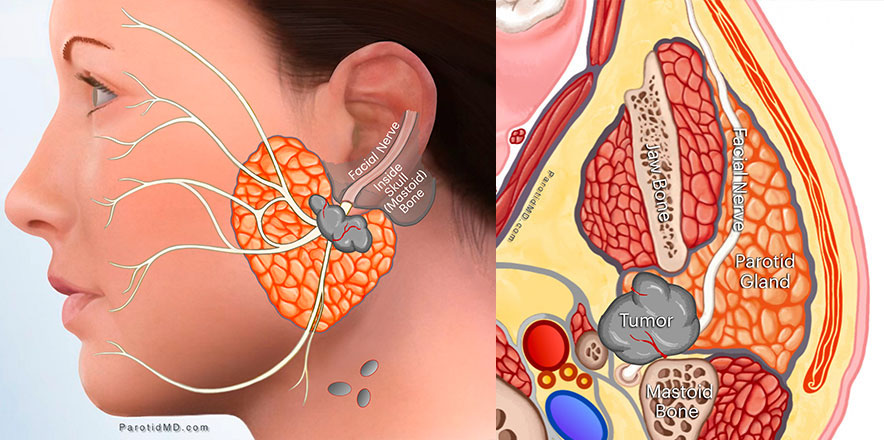
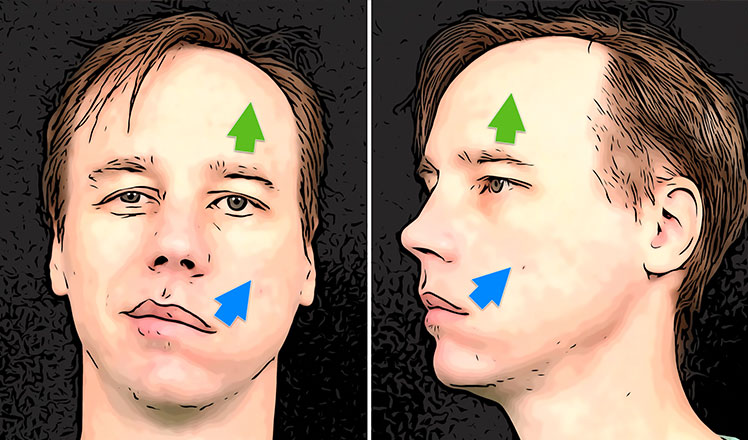
Cancers typically begin as painless lumps in the parotid gland, other salivary glands beneath the jaw, or within the mouth and throat. All masses should be promptly biopsied to determine if they are benign or cancerous. As the tumors grow, they can damage nerves, causing pain and paralysis. A parotid mass that is either painful or accompanied by facial weakness is very likely to be a cancer. Each type of cancerous tumor in the salivary glands has different characteristics and behavior patterns. The type of surgery & extent of treatment can be very different for each type. As such, salivary cancers require immediate attention by an expert team of salivary specialists. In this section, we briefly discuss some of the more prevalent types of salivary cancers. Please schedule a consultation with our expert physicians at the CENTER. You can either visit our office or have a video (Zoom) appointment to review your pathology report, examine your scans (which can be electronically sent to us in advance of the appointment), and discuss your personalized treatment plan in detail. We are here to help you!
MUCOEPIDERMOID CARCINOMA
Mucoepidermoid carcinoma (MEC) is the most common type of parotid gland cancer in both adults and children. Despite this, it is still a very uncommon cancer. Mucoepidermoid carcinoma is more common in women in the middle ages. Like all salivary cancers, it starts from an alteration in the DNA of a cell in the salivary gland. This mutated/altered cell continues to duplicate & grow, and as it grows, mutates more, losing more inhibitions & becoming more aggressive. MEC can be low grade, intermediate grade & high grade. Low-grade MEC tends to be more cystic & have more mucus cells which form glandular structures, while high-grade tumors are more cellular, less cystic, with a lot of atypical cells (they don’t look like a salivary gland anymore).
The low-grade mucoepidermoid carcinomas tend to be slow growing with a very low chance of spread, and usually require complete excision with only a limited parotidectomy for cure. The intermediate MECs tend to be slightly more aggressive with a slightly higher chance of spread to lymph nodes. Treatment for low-grade and smaller intermediate-grade tumors is just a parotidectomy with the removal of a small amount of additional salivary tissue around it. For larger Intermediate tumors, removal of the lymph nodes in the neck below the parotid gland is also considered.
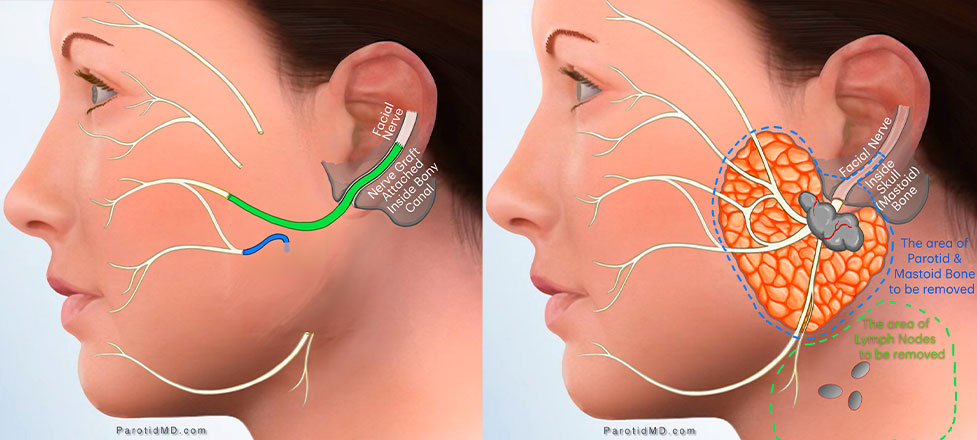
High-grade mucoepidermoid carcinomas have a lot more genetic alterations/mutations (genetic errors due to toxin/radiation exposures), which makes them grow faster & behave more aggressively. They are more likely to invade what is around them and spread to the lymph nodes. Consequently, prompt treatment with surgery (parotidectomy and lymph node removal in the neck, known as neck dissection) is essential. This is often followed by radiation therapy, and in some cases, additional treatments may be necessary. Signs of advanced disease are spread to lymph nodes, involvement of nerves, involvement of vessels (lymphovascular invasion), or a tumor coming out of the parotid gland and invading adjacent tissue (muscle, bone, or skin).
To determine the extent of the tumor and develop an appropriate treatment plan, imaging studies are crucial. Early diagnosis and prompt treatment by a parotid specialist are vital for achieving the best possible outcomes. If you have been diagnosed with MEC, please contact us at the CENTER to start prompt treatment.
ADENOID CYSTIC CARCINOMA
A very unusual cancer that can grow in glandular tissue all over the body, including salivary glands, breasts, tear glands, prostate, trachea & other areas. Adenoid cystic carcinoma (ACC) happens most often in the 5th & 6th decades of life, and occurs equally in women & men. Interestingly, it is the most common salivary gland cancer in the African continent. In the US, it is diagnosed in roughly 1300 people a year. It comes in three histologic (under the microscope) forms: tubular, cribriform & solid. The more solid the component seen under the microscope, the more aggressive the cancer’s behavior.
ACC is a slow-growing cancer that likes to penetrate surrounding areas and especially loves nerves. It uses nerves as a highway to travel to other areas. Once it has gotten onto the nerves, it becomes more difficult to treat because the nerves don’t have any boundaries to spread, so once ACC has gotten on a nerve, it can go from the parotid forward into the face or upwards into the brain. The key is early diagnosis and surgery before it has had a chance to spread to nerves or other parts. Even when it spreads, it still grows slowly (which is a very unusual characteristic). These cancers are defined by MYB or MYLB1 genetic alterations, which means the diagnosis can be confirmed by the presence of these abnormal genetic changes.
In the early stages, ACC presents as a painless lump in the parotid or anywhere in the mouth, but as it advances and involves nerves, it becomes painful and can cause paralysis. In the case of the parotid gland, it can cause facial nerve paralysis. Early tumors can often be treated & cured by surgery alone or in combination with radiation treatment. Advanced tumors are difficult to cure & like to spread to lungs, bones & liver, making early detection and treatment critical. Once treated, the person must be followed up for many years by their doctors, as they may recur years later.
Unfortunately, radiation treatment alone cannot get rid of ACC. Chemotherapy has not proven effective in curing ACC, but it may slow down the progression. Alternative therapies are continually being investigated, and clinical trials are always ongoing for this unusual cancer.
ACINIC CELL CARCINOMA
Acinic cell carcinoma is generally a slow-growing tumor. It can occur at any age, although it’s rare in children. It tends to affect a slightly younger population of patients compared to other salivary gland cancers. It has a predilection for people in their 40s and 50s and is slightly more common in women. It occurs more frequently in Caucasians than in other populations and is seen least often in people of African descent. It can run in families, and interestingly, in 3% of cases, it can be present in both salivary glands simultaneously. The only known risk factor is previous radiation exposure, such as radiation treatment for a medical condition.
Most often, Acinic Cell Carcinomas are low grade and don’t tend to spread unless not treated and given enough time to change and become more aggressive. In the early stages, they show up as a painless lump in the parotid or other salivary glands. Once they become more aggressive, they may start to hurt, grow more rapidly, invade surrounding tissue & nerves, and spread to other areas. The treatment, if caught early enough, is parotid surgery so that the entire tumor is removed along with an additional portion of healthy salivary tissue around it.
Rarely, acinic cell carcinomas are genetically very aggressive and eat through nerves, muscle, or skin. And equally rarely spread to lymph nodes. Pain, facial weakness, or enlarged lymph nodes show that the Acinic cell cancer is aggressive and will require more involved surgical treatment, and after surgery, radiation treatment.
CARCINOMA EX-PLEOMORPHIC ADENOMA
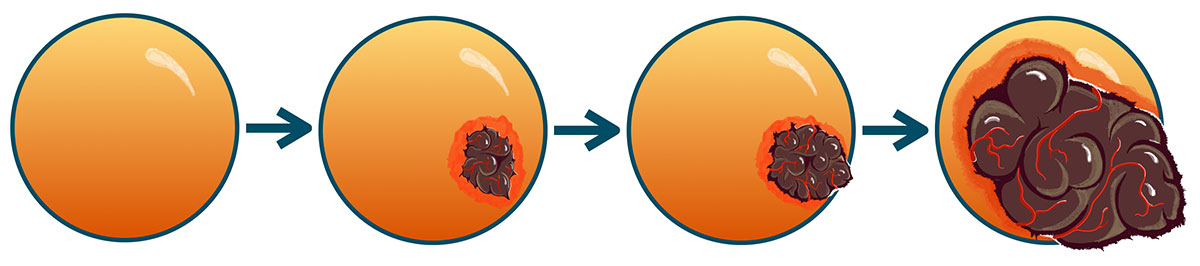
Carcinoma ex-pleomorphic adenoma or Ca-Ex-PA makes up roughly 10% of salivary gland cancers. It always arises or transforms from a benign pleomorphic adenoma that has not been removed or has recurred after incomplete surgery. The chance of a benign pleomorphic adenoma transforming into cancer is 1.5% at 5 years and 10% at 15 years, and unfortunately, the chance continues to increase with time. The transformation starts in one cell that turns into cancer. Then that cell starts to rapidly duplicate and get bigger. At first, the transformed cancer is small and exclusively inside the capsule of the pleomorphic adenoma. This is designated as non-invasive Ca-ExPA, since the cancer cells are not invading the capsule (the covering of the benign pleomorphic adenoma tumor). As the cancer grows, at some point it starts to eat through the capsule of the benign tumor, and grow out; when the cancer has grown out less than 1.5 millimeters, it is called minimally invasive carcinoma ex-pleomorphic adenoma. It will continue to grow more, and once beyond 1.5 millimeters, it is now called invasive Ca-Ex-PA.
Left to right: Pleomorphic Adenoma, Non-Invasive Carcinoma-Ex-PA, Minimally-Invasive Carcinoma-Ex-PA, Invasive Carcinoma-Ex-PA
Additionally, carcinoma ex-pleomorphic adenoma can take the form of any of the other salivary cancers, most commonly adenocarcinoma, epithelial-myopithelial carcinoma, or salivary ductal carcinoma. Whatever type of cancer it becomes, the level of aggressiveness will be similar to that particular cancer. So if the cancer is diagnosed at a non-invasive or minimally invasive stage and it happens to be a type that is relatively low grade, then surgery alone may be adequate as treatment. However, if the Ca-Ex-PA is invasive, a more aggressive type, or has spread to lymph nodes, it necessitates more extensive parotid surgery, lymph node removal, followed by radiation therapy, and potentially immunotherapy or chemotherapy. Post-surgery, specialized testing will be done to determine the exact cancer type and identify specific proteins that can be targeted for immunotherapy (targeted therapy).
This presents a particularly challenging scenario because it’s often uncertain whether the pleomorphic adenoma has transformed before surgery. The expertise of your surgeon greatly enhances the chances of detecting that the tumor has already transformed during surgery and taking appropriate action to address it. And also know how to plan an optimal treatment for you after surgery.
SALIVARY DUCTAL CARCINOMA
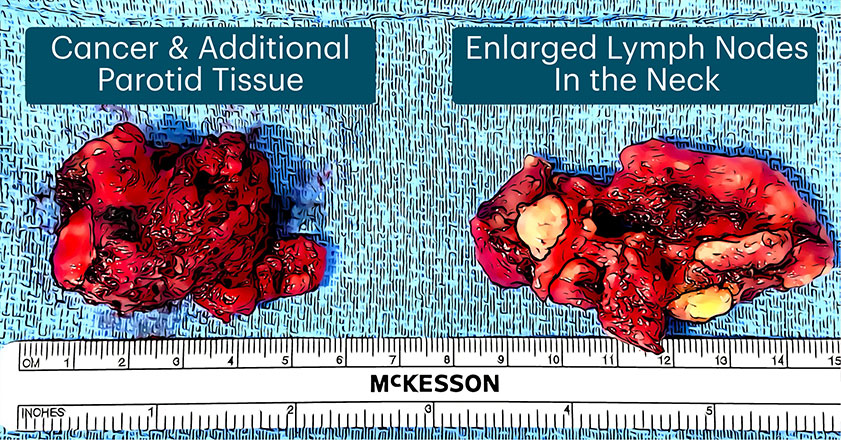
Salivary ductal carcinoma or SDC is a rare & aggressive cancer that occurs more commonly in men in the sixth & seventh decades of life. Interestingly, the incidence of SDC has been increasing in the past few decades. It happens most often in the parotid gland, followed by the submandibular gland. It commonly spreads to the lymph nodes. In fact, a great majority of patients with SDC initially go see their doctors because of enlarged lymph nodes in the neck and not necessarily because they find the original tumor in the parotid gland. SDC grows rapidly and, if left untreated, it can quickly invade any structure next to it, including paralyzing the facial nerve, or spread to other parts of the body.
Salivary ductal carcinoma can arise on its own or due to transformation from a benign pleomorphic adenoma. In either scenario, the progression of disease and treatment remains the same. SDC shares similarities with breast ductal carcinoma. Signs of advanced disease are spread to lymph nodes, involvement of nerves (facial weakness or paralysis), a larger tumor, high-grade histology, and spread to other organs (lung, liver, or bone). Greater then 70% of SDC have an androgen receptor on their surface, and roughly 30% have amplification of the HER2 gene, which is a target for immunotherapy. Treatment is almost always multi-modality, which means it will require surgery (parotidectomy with removal of neck lymph nodes – aka neck dissection), followed by radiation therapy, immunotherapy, androgen blockade, and/or chemotherapy. SDC is a very aggressive cancer that demands prompt intervention to prevent progression. Therefore, immediate action is of utmost importance.
There are many different types of Adenocarcinoma that occur in the salivary glands. Adenocarcinoma NOS (not otherwise specified) is the most common type in the parotid gland and will be discussed here. It is more common in older caucasian men, generally greater than 67 years of age. The grade of tumor can be determined by histologic features (findings under the microscope), with high-grade tumors acting more aggressively than low-grade ones. Indicators of aggressiveness in adenocarcinoma include a large tumor size, a tumor that is immobile or firmly attached to the surrounding structures, facial nerve weakness or paralysis, and the enlargement of lymph nodes.
Since Parotid Adenocarcinomas (NOS) are very aggressive and can very early on spread to the lymph nodes in the neck under the parotid, prompt treatment is needed. Needle biopsy can help diagnose the type of tumor, while imaging studies determine its size and extent. Surgery involves the complete removal of the cancer, along with an additional 1 cm of normal parotid tissue. Additionally, neck dissection is performed to remove any lymph nodes in the neck that may contain microscopic cancer cells. Post-surgery, radiation therapy significantly enhances the likelihood of cure and reduces the risk of recurrence in both the parotid gland and neck lymph nodes.
METASTASIS FROM OTHER CANCERS
Metastasis are cancer cells that have spread from the original site of a cancerous tumor to a different organ. When there is a metastasis, it indicates that the cancer has changed on a genetic level enough to be able to travel through the lymph nodes or blood vessels to other parts. The parotid gland has several lymph nodes within it. These lymph nodes are in charge of surveillance and filtration of the local area, including the skin of the side of the face, temple, scalp, and ear. As such, the great majority of metastasis to the parotid gland starts from skin cancers in the vicinity that travel through lymph vessels to get to the lymph nodes inside the parotid gland. Most of these metastases are squamous cell carcinomas, followed by melanomas. Needle biopsy will often be able to tell if it is a squamous cell carcinoma, but melanoma in the lymph nodes may not be as easily identified. Some of the cancers originating in the parotid gland may have a similar appearance on needle biopsy to a melanoma, making the distinction almost impossible.
Parotid squamous cell cancers are often preceded by a history of skin cancer that was removed some time in the past, or there may be one presently in an area that is not visible (like under scalp hair or beard). The treatment involves parotidectomy & removal of some of the lymph node groups in the neck that are associated with the parotid gland (called a neck dissection). Prior to this, a thorough investigation of the skin in the local area must be done to assess whether there is still any skin cancer remaining that may have to be removed as well. This is usually followed by radiation therapy for a much improved outcome.